‘If I Get Ill, It’s onto the Plane, and off to Poland.’ Use of Health Care Services by Polish Migrants in London
-
Author(s):Osipovič, DorotaPublished in:Central and Eastern European Migration Review, Vol. 2, No. 2, 2013, pp. 98-114Views: 16922
This paper explores a range of health care seeking actions adopted by Polish migrants living in London. It is based on the in-depth interviews with 62 Polish migrants who resided in London in 2007 and 2008. The study reflects experiences of a diverse group of participants encompassing individuals of different ages, family circumstances and employment statuses. It uncovered a number of actions such as avoiding contact with any health services, self-medication, utilising Polish private doctors in London, and accessing public health services in Poland and London. These services and strategies were often used successively, concurrently or interchangeably depending on individual’s assessment of their situation and circumstances at the time of experiencing a particular medical need. The research uncovered a prominence of transnational health care seeking practices as most participants continued to access at least some form of health care in Poland. It also noted the impact of the length of stay, knowledge of English and labour market position on patterns of health care use. Engagement with the British National Health Service (NHS) was characterised initially by lack of knowledge of the system resulting in meandering between different institutions. There was also a sense of cultural unease and mismatch of expectations characterising doctor-patient encounters. However, the pathways of access and attitudes towards the NHS began to change as migrants learned their way through the English health care system. This underlines an importance of taking into account a longitudinal dimension in studies of migrant health care seeking behaviour.
Introduction
Despite finding many common patterns in the way recent migrants engage with health care services in the host countries, empirical studies have struggled to provide a comprehensive and systematic conceptualisation of migrant health care seeking behaviour. Scholars distinguish two broad approaches in the literature on health care seeking behaviour – models addressing the pathways or series of steps that individuals take in search of medical help, and models concerned with specifying determinants of behaviour, both of which have come across major stumbling blocks (MacKian, Bedri, Lovel 2004). This paper discusses some of the challenges that remain in the way of such conceptualisations and aims to add to the growing body of empirical knowledge on migrant health care seeking actions in different health system contexts (see e.g. Leduc, Proulx 2004; Fassaert, Hasselink, Verhoeff 2009; Choi 2012).
Based on a qualitative study of Polish migrants’ engagement with the British welfare state, the paper outlines the rationales and consequences of utilising health care services during participants’ stay in London. The study followed the premises of grounded theory qualitative research (Glaser, Strauss 1967; Strauss, Corbin 1998 [1990]), therefore there were no a priori hypotheses set at the beginning of the fieldwork. Instead, the participants were selected in order to obtain a maximum diversity of socio-demographic characteristics, such as family circumstances and labour market position, based on the assumption that migrants in different circumstances may have different views and experiences of utilisation of public services in the UK. The broad question guiding the research pertained to the reasons for, experiences of, and consequences of utilising public services in Britain.
The large wave of post-2004 Polish migration to the UK has drawn a lot of attention from migration scholars, who began to gather empirical data on health status and health care experiences of Polish migrants in the UK. However, the existing studies of utilisation of health care services by Polish migrants in the UK rarely explore the rationales behind different behaviours and attitudes (although see Goodwin, Polek, Goodwin 2013; Migge, Gilmartin 2011 – in the Irish context). Furthermore, the health care seeking behaviours that fall outside of the host public health care system are seldom addressed. This paper aims to fill such gaps.
The paper outlines different health care options used by Polish migrants with accompanying rationales and examines how the condition of being a newcomer in a host society impacted engagement (and non-engagement) with the health services. It reflects upon some striking commonalities in patterns of engagement adopted by participants in this research and echoed in other studies of migrant health care seeking behaviour. At the same time, it pays attention to the diversity of behavioural responses within the studied group and behavioural change over time. The findings illustrate the challenges of generalising and conceptualising the accumulated empirical knowledge of migrant health seeking behaviour.
Theoretical maze of health care seeking behaviour
Health care seeking behaviour is a complex, socially- and culturally-embedded process. It is an example of human agency driven by individual health needs that is steered by social identifications and structural conditions that individuals face. Cultural norms, beliefs and attitudes formed as a result of past experiences of seeking medical help, including those acquired prior to arrival in the host country, play a role in directing actions in this respect (Leduc, Proulx 2004; MacKian et al. 2004). Moreover, structural or enabling factors such as working and living conditions, individual capabilities and capitals, as well as availability and accessibility of health care services also limit human agency.
Various studies highlight some striking similarities in the propensity and patterns of utilisation of health services by different migrant groups in different health care system contexts. Quantitative studies tend to report the underuse of services (both primary and secondary care) by immigrants compared to the settled populations; however, this effect tends to weaken or disappear with a prolonged length of stay (Leclere, Jensen, Biddlecom 1994; Steventon, Bardsley 2011). Some studies, predominantly conducted in the US context, attributed this finding to the effect of progressive acculturation usually measured by host language ability, adoption of host society’s norms and values, and social interactions with natives obliterating behavioural differences between immigrants and natives (e.g. Wells, Golding, Hough, Burnam, Karno 1989). However, others point out the problematic nature of the use of the acculturation concept as an explanatory variable of health behaviours and outcomes due to its vagueness and ideological bias (Hunt, Schneider, Comer 2004). Some researchers find little or no direct association between migrants’ level of acculturation and health service use and stress the heterogeneity of migrant groups, the importance of socio-economic barriers to health care use as well as the difficulty of disentangling the effects of length of stay, country of birth, ethnicity and language ability (Fassaert et al. 2009; Jayaweera, Quigley 2010). In particular, health care utilisation may be explained simply by the level of health needs, as the initial underuse of services may simply be due to the so-called ‘healthy migrant effect’, describing self-selectivity of migrants, resulting in lower morbidity and mortality rates compared to natives (e.g. Razum, Zeeb, Rohrmann 2000). Conversely, the weakening of this effect with the extended length of stay may be due to the ageing process.
It seems that using acculturation, or for that matter the more common in Western European literature concept of migrant integration, to explain health care utilisation is riddled with analytical problems. Such concepts seem too all- encompassing and contentious to serve as a helpful explanatory variable of human agency. Furthermore, these notions may be sociologically unsustainable as immigrants, much like everyone else, are always excluded and included at the same time in different fields of the host society, from the moment they set foot in a new country (Joppke, Morawska 2003: 3). Arguably, the notion of integration becomes meaningful only as an attribute of a particular society, and not of an individual. In such a sociological sense, outlined amongst others by Lockwood (1999), integration is achieved through the means of social citizenship, by individuals utilising their social rights, for instance by using public health care system. Therefore, the sociologically-grounded notion of integration can only be sustained as a consequence and a product of citizens’ actions, rather than their pre-requisite, as in theories of migrant integration or acculturation. As succinctly summarised by Sayad (2004: 223), integration can be achieved only as a side effect of actions undertaken for different purposes. This is not to deny that such factors as length of stay or language ability have an impact on health care seeking behaviour. Yet these factors can serve as a proxy for a number of social phenomena, not just ‘acculturation’ or ‘integration’ understood as a linear progression from one state to another. Furthermore, reverse causality is not only possible but plausible, as for instance the use of host health care services may lead to decisions to prolong the length of stay or to invest in learning the host language.
Arguably, one way out of such theoretical and explanatory mazes is offered by the human agency paradigm. It views health care seeking behaviour as reflexive and purposeful social action and puts an emphasis on the multiplicity and interdependency of factors potentially influencing such behaviour, be they individual, socio-cultural, economic, or structural in their origin, or even chance encounters or circumstances. Such a stance also stresses the human ability to learn from past experiences and draw on different cultural repertoires simultaneously in pursuit of goals (DiMaggio 1997; Swidler 1986). Qualitative studies of migrant health care seeking behaviour conducted in this vein seek to explore the reasons behind certain behavioural patterns, such as delay in seeking care, by situating such behaviours in migrants’ biographies and lifeworlds. Existing literature pays particular attention to structural barriers to health care utilisation, such as importance of cultural and linguistic appropriateness of health care settings, a lack of which may result in seeking alternative medicine, ethnic niche doctors or transnational care in the home country. It also stresses the importance of monitoring change in health care seeking behaviour over time (Leduc, Proulx 2004; Lee, Kearns, Friesen 2010; Migge, Gilmartin 2011). For instance, Leduc and Proulx (2004) distinguish three key stages of migrants’ engagement with the host health care system: contact, selection and consolidation. The authors find that length of stay is a crucial predictor of changes in health care seeking behaviour of recent immigrants. Increasing length of stay enables migrant individuals and families to learn how health services are organised in the host country and to select services based on evaluation of migrants’ first experiences with the host public health care system and any existing alternatives. This stage is followed by adoption of services that best suit them and formation of new utilisation habits (Leduc, Proulx 2004). The insights from existing qualitative literature suggest that despite some regularities in service utilisation patterns, the explanations of such patterns tend to be highly context specific.
Polish migrants in the UK and their health
There is a growing empirical literature on the conditions and consequences of the post-2004 wave of Polish migration to the UK. In 2013, the number of Polish citizens in the UK was estimated at 679 000, making them the largest foreign nationality group residing in the UK for several years running (Salt 2013: 50). Although the predominant motives of this migration were economic, Polish migrants constitute a diverse migrant group, including workers of low and average incomes, unemployed and homeless people, families with dependent children, and intergenerational households formed as a result of older people joining their adult children in the UK (see e.g. White 2011; Garapich 2011). Furthermore, researchers begin to note considerable upward social mobility of the post-2004 cohort of Polish migrants from entry level jobs to better paid occupations, perhaps as a result of capitalising on their relatively high levels of education (Goodwin et al. 2013).
The size, diversity and dynamism of this migrant group imply a wide spectrum of changing health needs. Although official British surveys show that Polish migrants are healthier on average than is the British general population,1 a number of studies pointed out considerable health needs of Polish and other Eastern European migrants, especially with regards to urgent care, maternity, paediatric care, sexual and mental health (e.g. Leaman, Rysdale, Webber 2006; Weishaar 2008; Lakasing, Mirza 2009; Evans, Mercer, Parutis, Hart, Mole, Gerry, Burns 2011). A longitudinal, multimethod study investigated the impact of various socio-demographic and acculturation variables on changes in health outcome perceptions of Polish migrants in the UK (Goodwin et al. 2013). In addition, researchers explored the level of satisfaction with the British National Health Service (NHS). They found that Polish participants were generally positive about administration of services and attention received from British clinicians, but less positive about clinicians’ competence and treatment received, especially in primary care settings. General practitioners (GPs) were described as the ‘paracetamol force’ due to participants’ conviction that they tend to prescribe paracetamol for all ailments (Goodwin et al. 2013:162). The study also found a widespread preference for transnational care, with 69 per cent of respondents stating that they would have preferred to receive medical treatment in Poland rather than the UK if money were no issue. Other cross-sectional studies investigating the use of the British NHS by Eastern European migrants reported low knowledge of the system at arrival, low take-up and delays in registrations with GPs, and differing patient expectations (e.g. Spencer, Ruhs, Anderson, Rogaly 2007; Collis, Stott, Ross 2010).
Polish migrants residing in London are able to access healthcare services from a number of sources. These encompass British and Polish public healthcare systems, private healthcare providers in London and Poland, and informal sources such as ethnic and transnational social networks offering information, care and medication. Poland operates a health insurance based system with comprehensive coverage of the resident population. However, as voluntary health insurance contributions are rare (Sagan et al. 2011: 69), the majority of non-statutorily insured Polish migrants (e.g. those with no employee or pensioner status in Poland) are mostly out of bounds of the Polish public healthcare system. In contrast, the British NHS is funded out of public taxation. It is available ‘free’ and unconditionally to all lawful residents of the UK regardless of their economic activity or payments of national insurance (DoH 2007).2 Thus, Polish migrants residing in the UK as European Union citizens are entitled to free NHS care.
Data and Methods
The paper draws on data collected as part of a doctoral study of the conditions and consequences of Polish migrants’ engagement with the British welfare state institutions (Osipovič 2010). The British NHS was one of the three areas of the welfare system taken into account, alongside social housing and non-contributory welfare benefits. In-depth interviews with 62 Polish citizens residing in London were conducted in 2007/2008.3 On a few occasions, members of the same household were interviewed jointly. The majority of interviewees (56 out of 62) had been in the UK for less than five years at the time of the interview. The sample was differentiated according to a number of socio-demographic and health characteristics, including labour market status and family circumstances (see Table 1).
Table 1. Selected characteristics of participants, (N = 62)
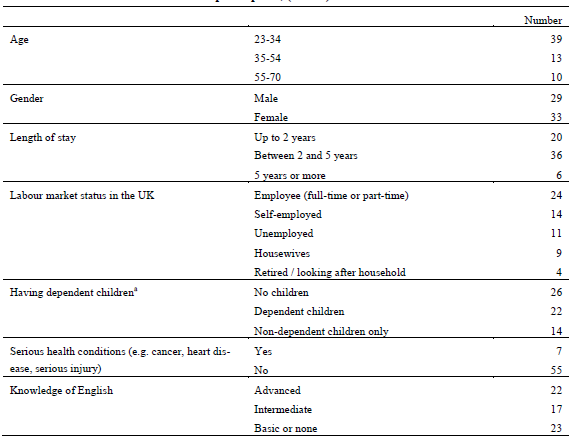
a Children under 16 or aged 16 to 18 in education.
Source: Polish migrants study 2007/2008.
Participants were recruited at various public gatherings and ethnic institutions such as play groups, job fairs, day centres and churches. Snowball sampling was generally avoided as the aim was for the sample to reflect diverse social circumstances that may have a bearing on migrants’ engagement with the host public services. Participants were informed of the aims of the research and their consent was obtained prior to the interview taking place. Table 2 below shows socio-demographic characteristics of participants quoted in this paper.
Table 2. Selected characteristics of participants quoted in the paper
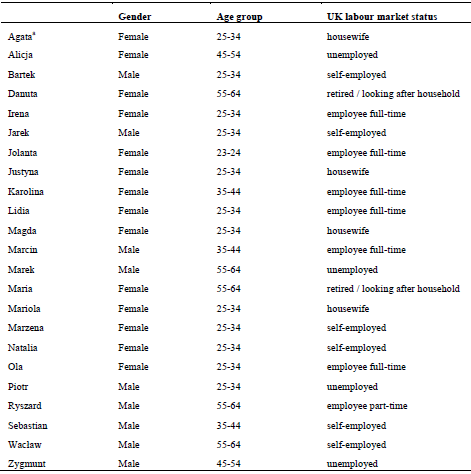
a All names of participants have been changed.
Source: Polish migrants study 2007/2008.
The fieldwork was guided by the broad research question of ‘why, how and with what consequences’ Polish migrants engage with British public services. The health care utilisation questions constituted a part of an interview schedule, which also addressed the usage of and attitudes towards other areas of the British welfare system. Participants were asked about their experiences of accessing any health care services during their stay in London, registration with a GP, sources of information about the NHS and their particular experiences of the NHS.
The grounded theory approach to data collection and analysis was adopted. This approach aims to reconstruct how individuals formulate and modify the meanings of actions, appreciate obstacles, and communicate with others (Glaser, Strauss 1967; Strauss, Corbin 1998 [1990]). The analysis evolved side by side with data collection, as new types of migrants with differential experiences and views were interviewed in the course of the fieldwork. The interviews were recorded, transcribed and analysed using multi-level coding with the help of Atlas.ti software. The interviews were conducted in Polish by the author who is a native speaker. The initial coding was performed in Polish, whilst the latter stages – in English. The core category that emerged from the data was the axis of (non)engagement with the host public health care system, with accompanying subcategories addressing conditions, actions, and consequences of (non)engagement (Strauss, Corbin 1998 [1990]: 125).
Findings
Coping without health care services
Similarly to other studies of migrant health seeking behaviour, this research exposed a tendency by some participants to delay seeking treatment or cope without resorting to formalised health care, especially at the outset of their stay. In the case of minor illnesses and ailments, self-medication and self-care was an option of first resort for the majority of participants, regardless of their living and working conditions. Many participants stored a collection of basic medicines, herbal remedies and even antibiotics brought from Poland just in case (Ola) or relied on local pharmacies.
However, more alarmingly, some participants who were seriously ill also delayed or avoided contact with the health care services. These were predominantly participants who were in casual, undocumented employment at the time and were avoiding contact with the NHS through fear of disclosure. Furthermore, some participants accustomed to the Polish health care system were unaware of the principle of unconditional access to health care in the UK, and anticipated rejection due to their undocumented employment status and non-payment of national insurance contributions. These concerns were particularly salient before 2004 EU enlargement, when denunciation could have resulted in deportation:
I don’t have any insurance or anything like that, I don’t pay taxes. Everything is linked, isn’t it? When you have insurance, then you are already registered, you can go to a doctor then, there are some services then. And because I don’t have it, you have to sit quietly (Ryszard).
Migrants in undocumented employment were also afraid of losing their jobs due to illness. Many such participants expressed a feeling of having ‘no time to be ill’, as their time was consumed entirely by working or looking for work. For instance, Marzena, who was doing some undocumented cleaning work at the beginning of her stay in London, reminisced:
At the beginning it was an ordeal, dear Jesus, because you were exhausted, you haven’t eaten properly, this and that, there were many times when I fell down the stairs with a Hoover, because I was exhausted; when you get ill (...) you apply home remedies, medicines sent from Poland, antibiotics, and you just go to bed after work, rest a couple of hours, and in the morning you get up and go to work again, this is how it was in those days.
Being time-poor and prioritising work and job searching above everything else made undocumented workers and those who engaged in documented but casual, intermittent employment unprepared for dealing with health crises as and when they occurred. For instance, Zygmunt, when asked why he was not registered with a GP at the time of a health crisis, replied: I have no time. Here everybody works hard to earn a living and that’s all.
Even among participants who had no language barrier and some knowledge of the NHS system, registering with a GP was not considered a priority in the initial period of stay in London, unlike finding a job and accommodation. This tended to change over time as nearly all participants who resided in London longer than two years at the time of the interview were registered with a GP, compared with only around half of participants who resided for less than two years. For instance, Piotr, who arrived with his girlfriend just one month before the interview took place, stated: We are not at this stage yet, we are absorbed by other things. We have other priorities. At some point we will definitely get around to doing this.
In one case, the delay in seeking help had fatal consequences. Two participants relayed the story of their housemate, an undocumented worker with no knowledge of English who relied entirely on his social networks and ethnic businesses for survival. When this person got seriously ill, his girlfriend apparently did not offer him any help (Lidia). The participants’ encouragement to visit an NHS doctor fell on deaf ears:
We kept telling him that he should get in touch, when he was still able to walk and was able to go to see
a doctor, to register with a [GP] surgery, we kept telling him that they will certainly provide him with an interpreter. I think that he was simply afraid, he was afraid of speaking any English at all.
Instead, the person relied on the advice of a Polish physiotherapist, but his condition, which was never properly diagnosed, gradually worsened. Eventually, the two housemates-participants phoned for an ambulance service. Despite these efforts, the person passed away shortly afterwards in an NHS hospital. Overall, the sole labour market focus, the language barrier and lack of information about the system, as well as a preoccupation with finding a job and accommodation were the crucial substantive barriers preventing newcomers from accessing NHS health care to which they were entitled.
Opting for ethnic private doctors in London
Polish health care professionals offering private services constituted a part of an ethnic niche economy catering to the large Polish community in London (Garapich 2008). There were several circumstances prompting participants to access help from private Polish doctors practicing in London – lack of information (or often misinformation) as to the set up and eligibility for the NHS, wariness of engagement with the NHS by undocumented workers, the language barrier, and a preference for a quick, culturally familiar service. Arguably, the fact that participants were used to paying privately for health care in Poland formed a habitual disposition facilitating such health care seeking behaviour.4
Many participants preferred to consult Polish doctors offering quick, culturally familiar service that, as a result, appeared trustworthy. Some participants sought a more medicalised approach to their complaints, expecting follow-up investigations and tests that they perceived as sometimes lacking in their encounters with NHS primary care services. Information about Polish doctors was widely available in the ethnic media and shops. Some, like Natalia, got in contact with a Polish doctor in London through her doctor in Poland:
I had minor surgery in Poland, I came back and I had to remove the sutures. My doctor from Poland gave me the contact details of a doctor here. He lives far away from me, in the south. I had to travel far. I made an appointment in the evening (...) he removed the sutures and told me what to do later, he was very nice... When I asked whether I can phone him if I have any problem, he said, ‘Yes, of course, no problem.’ So I have good experiences.
Not only were participants used to the concept of paying for health care as a result of their experiences in Poland, but purchasing health care services also fit with the commodified nature of everyday life in London’s migrant niche economy, where every service and favour had its price. The cost of services was a barrier to accessing health care from private doctors, as it was prohibitively expensive for migrant workers on low wages. As a result, such services were used sparsely and only in extreme circumstances when self-care failed:
I didn’t have much money to pay for a Polish doctor, the only time when I had a serious problem (...), I went to a Polish doctor, I knew that I wouldn’t manage myself this time, I needed an appropriate antibiotic, for this specific illness, so I went to a female doctor (...), she helped me, I paid £50 for professional help (Marzena).
Transnational commuting for health care
In contrast to the incidental use of private Polish doctors in London, accessing health services in Poland was done on a much larger and regular scale by the majority of participants. Participants arranged special trips to Poland to seek urgent, elective or preventative care, or fit in medical appointments during holidays or family visits. The majority of participants had no medical insurance in Poland and most of the services they accessed were covered by one-off, out-of-pocket payments. In most cases, participants continued to rely on private doctors and services that they used prior to moving to London.
There were several reasons for seeking health care in Poland. Many participants wanted fast and efficient help in a culturally familiar environment. Perceived drawbacks of the NHS also played a role in seeking out alternatives. Polish health care professionals were seen as trustworthy due to the established relationships between patients and doctors. Conversely, a dose of mistrust, unease and cultural unfamiliarity characterised participants’ interactions with NHS professionals. For instance, participants were dissatisfied with the waiting times to see GPs and specialists and sought second opinions to compare the advice offered by NHS doctors.
If I go to a GP here with a problem, and I have to wait two weeks, then I’d rather buy a ticket and go to Poland, and I will come back in a week and will be cured quicker than here (Bartek).
The anxieties about the perceived inadequacies of NHS care were especially heightened in cases involving children:
I got scared. There was a somewhat sluggish reaction here. (…) they did one, two tests, that was all. (…) so we took him for private treatment to Poland (Karolina).
As the speed of obtaining help was the main requirement for the majority of participants, even Polish pensioners such as Danuta, who was entitled to public health care system in Poland, opted to access care privately in order to get seen quickly and return to their household responsibilities in London:
In order to get an appointment with a [specialist doctor in Poland], you have to make an appointment (...), I don’t know, maybe two months in advance. When I go to Poland, I don’t have two months. To get
a referral for the ultrasound, to do an ultrasound, then again let them know, make an appointment with
a doctor to find out the results… so I am forced to do it privately.
Older participants who faced a language barrier often preferred to access the more familiar Polish health care system than the NHS, despite being entitled to both, especially when they were due to have a major procedure:
The doctor [in the hospital] told me that if I want they could do an operation. But I said, ‘Thank you very much, I don’t live here permanently. I will go to Poland and I will sort it there.’ (…) And shortly after that I went to Poland (…) and I had my operation in Poland (Maria).
Participants also accessed a range of services preventatively, including attending private specialists – such as dentists, ophthalmologists, gynaecologists – and conducting prophylactic and diagnostic tests such as blood tests and ultrasound scans: When we go there for two weeks, there is practically not a day without a visit to a doctor (…) we pay, all privately (Sebastian).
A few participants tried to use the European Health Insurance Card issued in Britain, designed to cover emergency care in the EU, to gain access to the Polish public health care system for non-urgent reasons with varied success. Perhaps due to the relative novelty of the card, some uninsured participants managed to obtain a free non-emergency consultation, whilst others were unable to do so.
Going to Poland was seen by migrant workers in casual employment who experienced an injury or accident at work as more cost-effective than staying in London for the recuperation period. This allowed them to minimise the loss of savings spent on costs of living in London without a steady income. As Wacław, a builder in his 50s, pointed out: if I get ill, it’s onto the plane, and off to Poland.
However, costs associated with seeking help in Poland were a major barrier for participants who faced financial difficulties in London whilst at the same time facing serious health problems. As a result, they could not afford the ‘beyond NHS’ strategies of shopping around for alternative or top-up care, even though they might have been dissatisfied with some aspects of NHS care:
In my current condition, I doubt that I can get free medical help [in Poland], certainly not. I don’t pay insurance premiums there. I could get help from possibly even better specialists than here, but I would have to pay a lot of money, which I don’t have (Alicja).
Transnational health care seeking was enabled by relatively low cost travel to Poland at the time, and the relative geographical proximity of Poland, which facilitated short trips and swift returns, a form of commuting for health care. However, those who routinely relied on accessing at least some services in Poland began to notice an increase in the costs of such commuting as the era of cheap air fares came to an end. As a result, some participants deemed accessing health care transnationally an unsustainable strategy in the long term and began to move their ongoing care from Poland to the NHS institutions.
Accessing NHS health care
There were several pathways and circumstances that led to participants’ engagement with the British public health care system. Universal access, decoupled from economic activity status and predicated on the ‘ordinary residence’ principle, allowed all participants, even those who were unable to document their involvement in the UK labour market, to use both primary and secondary NHS care free of charge. However, not all participants were aware at the outset of their eligibility to use the NHS and of how and where to obtain the care appropriate to their needs. Direct access services such as hospitals’ Accident and Emergency (A&E) departments, walk-in and ambulance services were often the first point of contact with the NHS.
The NHS often acted as an ultimate safety net for participants requiring urgent care, even if such participants also utilised non-NHS based health services at some point. In fact, it was not uncommon for participants to explore other options before turning to the NHS for help. For instance, Marek initially contacted a Polish private doctor in London who referred him for a number of diagnostic tests. Marek could not afford to pay the £368 bill, as he was earning about £240 per week at the time. He decided, after discussions with his family, to take advantage of cheap air tickets to fly to Poland and do all tests privately in Poland. The test results indicated that he required immediate treatment but having checked the waiting lists in the Polish public system to which he was entitled, he decided to return to London. He registered with a GP and was urgently referred for specialist NHS treatment.
Similarly, when Zygmunt began to experience health problems he went to a local pharmacy where a Polish-speaking pharmacist directed him to a nearby Polish private doctor. The participant visited this doctor three times, each visit costing £50, and was prescribed antibiotics, yet his condition worsened and may not have been diagnosed properly in the first place:
The woman from the pharmacy told me, ‘Zygmunt, don’t go there anymore, because he will kill you off with these antibiotics, (...) go to emergency and tell them how you feel.’ What can I say? I took this silly phrasebook for emigrants, what other choice did I have? I told them that I am out of breath, I showed them. I came across a Polish woman, she was with her father (…). I asked her whether she could come in with me and tell them what was wrong with me. And she did. They told me to wait a few minutes, somebody came from the hospital and took me in. I remember this much, they put me in a bed and put a drip in. And I don’t remember anything else.
Another participant went through a fairly typical meandering between various direct access NHS services before discovering the best routes (Lidia) of accessing specialist care. After experiencing a severely twisted limb, Lidia contacted an ambulance service, which directed her to the local walk-in clinic, which in turn sent her to the hospital A&E. However, upon discharge from A&E, her condition did not improve and she finally decided to register with her local GP. The following dialogue between Lidia and her same-sex partner Irena exposes the process of evaluation and learning from their experiences:
If something happens again then we will go straight to a GP, we will avoid the Walk-in Centre. We do not trust this institution. [We won’t go] directly to the hospital either, because you get admitted to the emergency ward and the things that happen there are also horrific, one leaves there ill (Irena).
Well, the route through a GP is definitely the best. At least my experience was such that the woman [GP] acted very fast. Not only did I see an orthopaedist the same day, I saw two of them. This was the fulfilment of all my dreams at that moment (Lidia).
For participants with limited knowledge of English, networks of co-ethnics were the main sources of information about the NHS. However, these networks were also a source of misinformation and negative stereotypes about the NHS. For instance, there was a widespread conviction that doctors are not willing to prescribe anything apart from paracetamol (Ola), which together with other common pain killers were referred to ironically as the miracle drugs (Lidia) in a number of interviews. Some negative stereotypes about the NHS were so entrenched that in some cases they were not even shaken by good first-hand experiences of the NHS, which were put down to luck. On the other hand, young, well-educated participants were wary of information spread through Polish social networks and preferred to obtain information about the NHS (and other British institutions) directly from British sources. This required a degree of linguistic and civic competences. For instance, Mariola recalled the way she went about registering with a GP: I popped into the first encountered [GP] surgery and they gave me an internet address and then I phoned some surgeries where they have places and… I went and registered.
Although participants who did not know English and had limited knowledge of the NHS system had far greater communication problems in encounters with NHS professionals, even those for whom language was not a barrier felt some unease resulting from the clash of health cultures and expectations, a feeling that something isn’t right with the health care here, as Maria put it. For instance, participants often expected a more medicalised approach from primary care professionals. Furthermore, some participants were baffled by the patient-centred discourse that doctors employed to encourage patients to arrive at shared diagnostic and treatment decisions. This was often perceived as a sign of a doctor’s incompetence:
I don’t ever recall a doctor back home, taking their books out and checking. They must have it all in their heads, that’s how it is. And here (the GP) takes a book out and says, ‘Listen, I can prescribe this, this or that. Have you chosen something?’ (Marcin).
Similarly, expectations of more medicalised care during pregnancy caused some initial anxiety to pregnant women:
At first it felt very odd to me, for example you don’t visit a gynaecologist during pregnancy, (...) back home you do every month and generally every two months there are tests and here – nothing. And I thought, ‘God, what if something is wrong?’ (Justyna).
At the same time, participants often had some ideas themselves as to what tests they should be offered or what diagnoses they could expect. As Jolanta remarked: people simply know what they may suffer from even before they go to doctor. As a result, some participants were fairly argumentative and refused to have ‘blind faith’ in doctors (Jolanta). For instance, Agata argued with a doctor about the normal body temperature of her child: She said that 37 degrees is a normal (body) temperature, I said, ‘No, this is not a normal temperature, 36.6 is normal.’
On many occasions, respondents stressed that assertiveness, persistence and psychological stamina is required in contacts with the NHS, especially when asking for referrals to specialists or diagnostic tests:
You have to fight here for some things, you have to say that you want something to be done and you have to sort it out because doctors here don’t know that… hmm… that such matters should be sorted out (Mariola).
Arguably, the sense of unease that some participants experienced in contacts with the NHS combined with a lack of docility on their part contributed to participants looking for private and transnational options of accessing medical help. Nevertheless the NHS played a crucial safeguarding role in providing access to health care for individuals who otherwise would not have been able to purchase it privately either in Britain or in Poland or who were not eligible to use the Polish healthcare system. This openness and ‘humaneness’ of the NHS (Marcin) was praised by a number of participants. Furthermore, the initial wariness was dissipating (albeit slowly) and participants began to notice positive aspects of the NHS as they became familiar with the new health care system.
Discussion and conclusion
The study showed that health care seeking behaviour is a process that unfolds within individual biographies. Rather than relying solely on one option, participants tested different strategies, used them concurrently, interchangeably or successively, and sometimes changed their minds presenting a multifaceted and ‘messy’ picture of health care service utilisation by recent Polish migrants to the UK. The transnational connections and the reliance on privately paid services featured prominently alongside utilisation of the NHS services. One can conclude that participants’ decisions to engage or not with the NHS were an outcome of reflexive assessment of their means and preferences set within the context of transnational and private health care alternatives. The wide range of observed health care seeking pathways exemplifies the difficulties of generalising these patterns onto the whole migrant population. This explains why thus far there has been mixed evidence of the extent to which Polish migrants use the NHS, with some studies reporting low take-up and others pointing out considerable needs and use.
Many health care seeking patterns, such as avoidance of care by undocumented workers, low priority assigned to preventive care, trips to Poland to recuperate, were intrinsically linked with the host labour market position of the participants. Thus, one can argue that the employment situation of economic migrants has a profound impact on their health care seeking pathways. Similarly, the study found an impact of the length of stay on health care seeking behaviour, in particular a move from reliance on direct access, emergency type NHS services to registration with general practices and more appropriate use of services. Lack of English knowledge was another important factor limiting sources of information about the NHS to Polish migrants’ networks and steering individuals towards looking for ethnic clinicians practicing in London or in Poland.
The study noted some change in health care seeking behaviour of Polish participants. In this sense it concurs with studies suggesting that migrants’ low take-up of GP registrations and high reliance on emergency care may be temporary phenomena, characterising initial stages of migration (Leduc, Proulx 2004). As most of the participants were relative newcomers, one can expect that the stage of meandering between different health care services and first inappropriate encounters will be followed by the stage of ‘consolidation’, whereby upon evaluation and reflection migrants establish regular sources of health care (Leduc, Proulx 2004: 23). These, however, may or may not be based within the host public health care system, as many participants also utilised medical services outside of the NHS.
The cross sectional nature of this study presents some limitations. Although I was able to trace some changes in behaviour retrospectively, a longitudinal study design is required to further explain the circumstances of behavioural change. Furthermore, findings of this study may be limited to the London area, with its concentration of health services as well as the presence of an ethnic niche economy. Other patterns may emerge as relevant in small town or rural settings. The timing of the fieldwork meant that the participants had not yet experienced the full effects of the financial crisis that hit the UK and London economy in 2008. It might have reduced the affordability of certain strategies, such as commuting for health care to Poland or reliance on private doctors in London.
The studies of health care seeking behaviour, and especially migrant health care seeking behaviour, pose considerable analytical challenges. The usage of the notions of acculturation or (migrant) integration as explanatory variables is surrounded by controversies. Although this study found an important influence of length of stay, English knowledge, and labour market position on health care seeking patterns, treating these factors as indicators of acculturation or integration may be akin to adding unnecessary ideological baggage to something that should be taken at face value as indicators of passing time, knowledge of foreign language and one’s way of earning a living. Especially in the case of length of stay, it remains difficult to hypothesise the actual causal mechanisms and processes that may be responsible for the impact that length of stay has on behavioural change as far as health care seeking is concerned. Furthermore, such factors themselves remain in flux, and their impact is not deterministic as, for example, even those who did not speak the language made use of the NHS in emergency situations. The issue of potential reverse causality, in that for instance reliance on host health care services can influence one’s decision to prolong the length of stay, further complicates the search for factors involved in influencing health care seeking behaviour. It seems that any explanatory mechanisms must reflect social practices and remain close to migrants’ everyday experiences.
On the other hand, the theoretical perspective of human agency adopted in this paper is also not capable of providing a definitive, general model of migrant health care seeking behaviour. The definition of health care seeking behaviour as social action is tautological in its nature. It stops at recognition and acceptance that actions of individuals are messy and complex and escape attempts to compartmentalise them. Partly because of this blind alley, some scholars of health seeking behaviour advocate a turn away from a focus on the individual toward group and collective levels, for instance by re-examining the concepts of reflexive communities and social capital (MacKian et al. 2004). Yet arguably the usage of such concepts as explanatory factors of individual behaviour may lead to a similar trap of social determinism that acculturation-based explanations have fallen into. Although undoubtedly collective variables, such as social capital, influence behaviour, ultimately it is the individual who seeks medical help. He or she is capable of assessing the options, learning from experiences and changing the course of action accordingly, as demonstrated by some participants in this research. Therefore, explanations of health care seeking behaviour must strike a balance between over- and under-socialised views of the individual.
The changeable nature of health care seeking patterns of new migrants has some implications for health care providers and health services research. In order to understand the assumptions that migrants approach the host health services with, health care providers have to show a dose of cultural sensitivity, flexibility and reflexivity. One has to recognise not only the cultural baggage migrants are coming with, but also the learning and evaluative processes that result in change of attitudes and preferences. This requires a shift from a focus on immediate issues and pressures that health services face to a more long-term perspective in planning services, in order to ensure that services are able to adapt to migrants’ changing preferences and needs. The adoption of longitudinal study designs may help in achieving such tasks.
Key messages
- Polish migrants in the UK utilised a variety of sources of medical help, including self-care, private ethnic doctors in the host country, private and public health care systems in the home country and the host country’s public health care system.
- The same individuals combined health care from different sources.
- The patterns of engagement with the host public health care system changed over time from an ad hoc reliance on direct access services to registration with primary care clinicians and more appropriate use of services.
- It is crucial to include the aspect of change over time in studies of migrant health care seeking behaviour.
Acknowledgements
This paper draws on findings from the doctoral research project Social citizenship practices of Polish migrants in London. The research was supported by the UK CEELBAS/ESRC doctoral studentship, which I gratefully acknowledge. I would like to thank the participants for their time and willingness to share their experiences. Also I am grateful to Judith Green and Andrew Wallace for their helpful comments on early drafts of this paper. Finally, I would like to thank two anonymous referees for their constructive input in improving the paper.
Notes
1 Data from the 2007/8 UK Labour Force Survey show that only 2% of working age Polish citizens reported some degree of long-term health problems, compared with about 20% of working age British citizens (Osipovič 2010).
2 Access to the NHS is predicated on the ordinary residence principle. A person is deemed ordinarily resident when it is established that he or she is living lawfully in the United Kingdom voluntarily and for settled purposes as part of the regular order of their life for the time being, whether they have an identifiable purpose for their residence here and whether that purpose has a sufficient degree of continuity to be properly described as ‘settled’ (DoH 2007: 18).
3 As the original research questions pertained to a large chunk of the British welfare state (not just health care), it was considered necessary to conduct quite a large number of interviews. In total, 50 interviews with 62 individuals were conducted as part of this study.
4 Out-of-pocket payments represented around 27% of total health expenditure in 2008 in Poland, which exceeded the level seen in most other EU member states (Sagan et al. 2011: 55-58). A large proportion of these payments covered the costs of medicines. Yet, arguably, there is also a culture of reliance on private specialist consultations, diagnostics and preventative care. As Kazik noted, in Poland we have such a [health care] system that everything is done privately.
References
Choi J. Y. (2012). Negotiating Old and New Ways: Contextualizing Adapted Health Care-seeking Behaviors of Korean Immigrants in Hawaii. Ethnicity & Health 18(4): 350-366.
Collis A., Stott N., Ross D. (2010). Workers on the Move 3. European Migrant Workers and Health in the UK: The Evidence. Thetford: Keystone Development Trust.
DoH (2007). Implementing the Overseas Visitors Hospital Charging Regulations Guidance for NHS Trust Hospitals in England. Department of Health. Online: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicati... (accessed: 28 February 2010).
DiMaggio P. (1997). Culture and Cognition. Annual Review of Sociology 23: 263-287.
Evans A. R., Mercer C. H., Parutis V., Hart G. J., Mole R., Gerry C. J., Burns F. M. (2011). Factors Associated with Genitourinary Medicine Clinic Attendance and Sexually Transmitted Infection Diagnosis Among Central and East European Migrants in London. Sexually Transmitted Infections 87(4): 331-336.
Fassaert T., Hesselink A. E., Verhoeff A. P. (2009). Acculturation and Use of Health Care Services by Turkish and Moroccan Migrants: A Cross-Sectional Population-based Study. BMC Public Health 9(332).
Garapich M. P. (2008). The Migration Industry and Civil Society: Polish Immigrants in the United Kingdom Before and After EU Enlargement. Journal of Ethnic and Migration Studies 34(5): 735-752.
Garapich M. P. (2011). Of Alcohol and Men – Survival, Masculinities and Anti-institutionalism of Polish Homeless Men in a Global City. Studia Migracyjne – Przegląd Polonijny 37(1): 309-330.
Glaser B. G., Strauss A. L. (1967). The Discovery of Grounded Theory: Strategies for Qualitative Research. Hawthorne, N.Y: Aldine de Gruyter.
Goodwin R., Polek E., Goodwin K. (2013). Perceived Changes in Health and Interactions with ‘the Paracetamol Force’: A Multimethod Study. Journal of Mixed Methods Research 7(2): 152-172.
Hunt L. M., Schneider S., Comer B. (2004). Should ‘Acculturation’ Be a Variable in Health Research? A Critical Review of Research on US Hispanics. Social Science & Medicine 59(5): 973-986.
Jayaweera H., Quigley M. A. (2010). Health Status, Health Behaviour and Healthcare Use Among Migrants in the UK: Evidence from Mothers in the Millennium Cohort Study. Social Science & Medicine 71(5): 1002-1010.
Joppke C., Morawska E. (2003). Integrating Immigrants in the Liberal Nation-States, in: C. Joppke, E. Morawska (eds), Toward Assimilation and Citizenship: Immigrants in Liberal Nation-States, pp. 1-36. Basingstoke, New York: Palgrave Macmillan.
Lakasing E., Mirza Z. A. (2009). The Health of Britain's Polish Migrants: A Suitable Case for History Taking and Examination. British Journal of General Practice 59(559): 138-139.
Leaman A. M., Rysdale E., Webber R. (2006). Use of the Emergency Department by Polish Migrant Workers. Emergency Medicine Journal 23(12): 918-919.
Leclere F. B., Jensen L., Biddlecom A. E. (1994). Health-care Utilization, Family Context, and Adaptation Among Immigrants to the United States. Journal of Health and Social Behavior 35(4): 370-384.
Leduc N., Proulx M. (2004). Patterns of Health Services Utilization by Recent Immigrants. Journal of Immigrant Health 6(1): 15-27.
Lee J. Y., Kearns R. A., Friesen W. (2010). Seeking Affective Health Care: Korean Immigrants' Use of Homeland Medical Services. Health & Place 16(1): 108-115.
Lockwood D. (1999). Civic Integration and Social Cohesion, in: I. Gough, G. Olofsson (eds), Capitalism and Social Cohesion. Essays on Exclusion and Integration. New York: Macmillan Press Ltd.
MacKian S., Bedri N., Lovel H. (2004). Up the Garden Path and Over the Edge: Where Might Health-seeking Behaviour Take us? Health Policy and Planning 19(3): 137-146.
Migge B., Gilmartin M. (2011). Migrants and Healthcare: Investigating Patient Mobility Among Migrants in Ireland. Health & Place 17(5): 1144-1149.
Osipovič D. (2010). Social Citizenship of Polish Migrants in London: Engagement and Non-engagement with the British Welfare State. PhD thesis. London: UCL. Online: http://discovery.ucl.ac.uk/20186/ (accessed: 29 January 2014).
Razum O., Zeeb H., Rohrmann S. (2000). The ‘Healthy Migrant Effect’– Not Merely a Fallacy of Inaccurate Denominator Figures. International Journal of Epidemiology 29(1): 191-192.
Sagan A., Panteli D., Borkowski W., Dmowski M., Domański F., Czyżewski M., Goryński P., Karpacka D., Kiersztyn E., Kowalska I., Księżak M., Kuszewski K., Leśniewska A., Lipska I., Maciąg R., Madowicz J., Mądra A., Marek M., Mokrzycka A., Poznański D., Sobczak A., Sowada C., Świderek M., Terka A., Trzeciak P., Wiktorzak K., Włodarczyk C., Wojtyniak B., Wrześniewska-Wal I., Zelwiańska D., Busse R. (2011). Poland: Health System rRview. Health Systems in Transition 13(8): 1-193.
Salt J. (2013). International Migration and the United Kingdom: Report of the United Kingdom SOPEMI Correspondent to the OECD, 2013. London: MRU.
Sayad A. (2004). The Suffering of the Immigrant [La double absence: Des illusions de l'émigré aux souffrances de l'immigré]. Cambridge: Polity Press.
Spencer S., Ruhs M., Anderson B., Rogaly B. (2007). Migrants' Lives Beyond the Workplace. The Experiences of Central and East Europeans in the UK. York: Joseph Rowntree Foundation.
Steventon A., Bardsley M. (2011). Use of Secondary Care in England by International Immigrants. Journal of Health Services Research & Policy 16(2): 90-94.
Strauss A. L., Corbin J. (1998 [1990]). Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. 2nd ed. London: Sage Publications.
Swidler A. (1986). Culture in Action: Symbols and Strategies. American Sociological Review 51(2): 273-286.
Weishaar H. B. (2008). Consequences of International Migration: A Qualitative Study on Stress Among Polish Migrant Workers in Scotland. Public Health 122(11): 1250-1256.
Wells K. B., Golding J. M., Hough R. L., Burnam M. A., Karno M. (1989). Acculturation and the Probability of Use of Health Services by Mexican Americans. Health Services Research 24(2): 237-257.
White A. (2011). Polish Families and Migration Since EU Accession. Bristol: Policy Press.